











 156 / 492
156 / 492

08:06 - 08:09
S12-3
(PP)
★
RISK FACTORS FOR FISTULA FORMATION AFTER DISTAL AND MIDSHAFT TIP
REPAIR: A COMPREHENSIVE TIME TO EVENT ANALYSIS OF 1267 PATIENTS
Soojin KIM
1
, Luis BRAGA
1
, Jennifer DCRUZ
1
, Kizanee JEGATHEESWARAN
1
, Jorge DEMARIA
1
, Armando J. LORENZO
2
and
Joao L. PIPPI SALLE
3
1) McMaster University - McMaster Children's Hospital, Department of Surgery / Urology, Hamilton, CANADA - 2)
Hospital for Sick Children, Department of Surgery / Urology, Toronto, CANADA - 3) Sidra Hospital, Department of
Surgery / Urology, Doha, QATAR
PURPOSE
To identify risk factors for urethrocutaneous fistula(UCF) after adjusting for confounders in a large multi-surgeon,
prospective cohort of midshaft/distal tubularized incised plate(TIP) repairs.
MATERIAL AND METHODS
Between 2008-2014, 1267 children who underwent distal/midshaft TIP repair by 6 surgeons were prospectively
followed. Proximal defects, redos and those receiving testosterone were excluded. Primary outcome was time-to-UCF
rate. Eight a priori defined risk factors were explored:age at surgery[</>1yr], glans groove[moderate/deep
vs.shallow/no], meatal location[distal vs.midshaft], chordee correction[>30
o
], suture type[polydioxanone
vs.polyglactin], urethroplasty(UP) layers[1vs.2], coverage layer[dartos/spongioplasty vs.neither], and stent insertion.
Cox-proportional hazard model was used to evaluate associations between risk factors and time-to-UCF.
RESULTS
Median age at surgery was 14(6–325)months; 15(1%)pts were post-pubertal; 1123(87%) had distal defects. Median
follow-up time was 23(2–92)months. Overall, 8%(97/1267) developed UCF at median time of 6(3–55)months. Mean
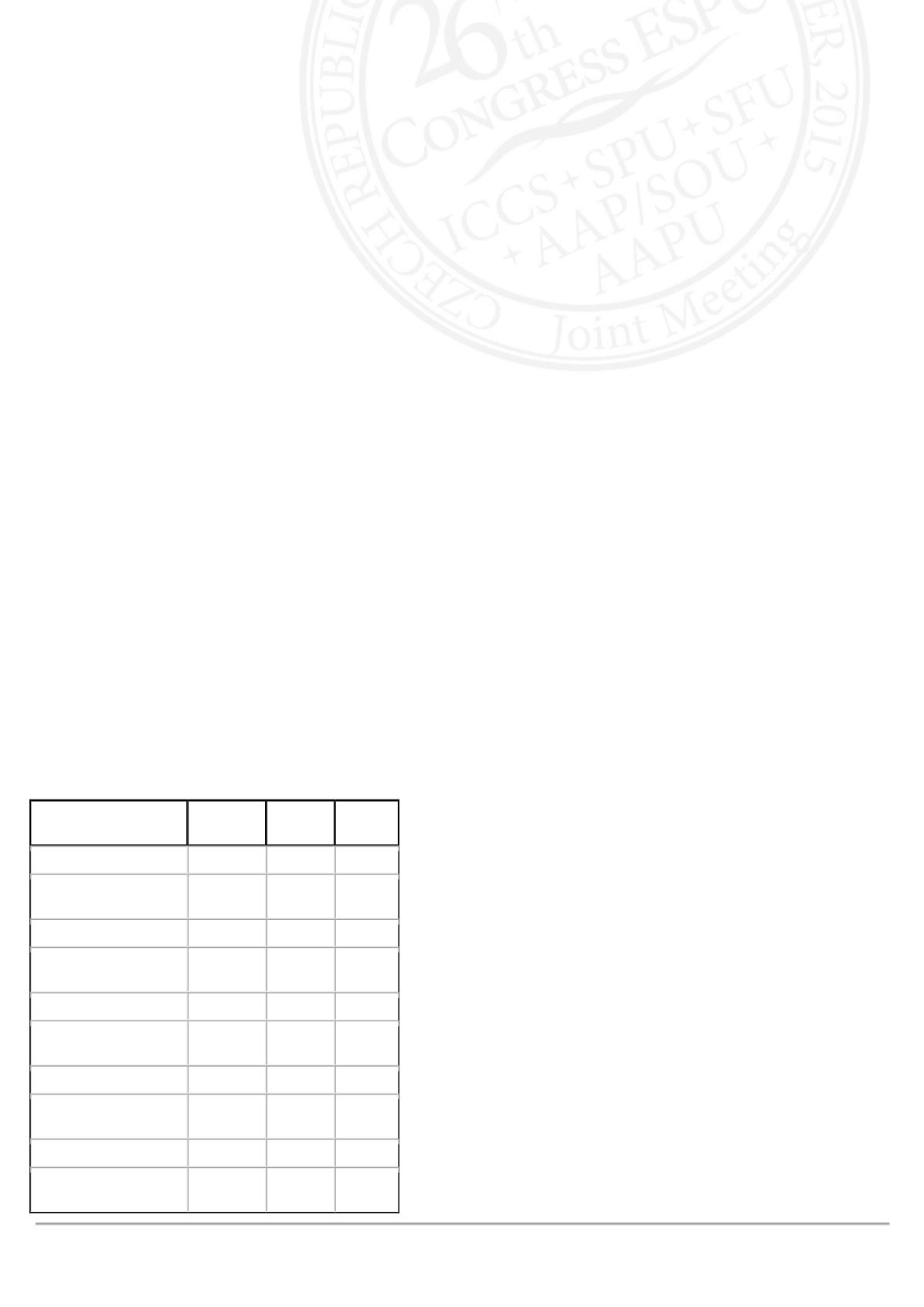
age at surgery was similar between patients with vs. without UCF(21.6±23.2 vs.21.3±24.8,p=0.9). Table 1 shows
univariate analyses. Shallow/no glans groove(HR=4.7,p<0.01), 1–layer UP(HR=1.9,p=0.04), and lack of UP
coverage(HR=2.2,p=0.02) were found to be independent risk factors for UCF on multivariable analysis. Older
age(>1year), midshaft defects, chordee correction and stenting were not associated with higher UCF rate.
CONCLUSIONS
This large, properly powered cohort study demonstrates important risk factors for UCF, two of which (UP layer and
coverage) are modifiable and under surgeons' control.
Table 1:Univariate Analysis of Risk Factors for UCF
Risk Factor
Fistula
N=97(%)
Total
N=1267
p-value
Glans Groove
<0.01
Moderate/Deep
Shallow/No
57(6)
40(14)
975
292
Suture Type
<0.01
Polydioxanone
Polyglactin
54(6)
43(11)
869
398
Urethroplasty Layers
0.03
2
1
16(5)
81(9)
328
939
Coverage Layer
0.02
Yes
No
86(7)
11(15)
1193
74
Stenting
0.04
Yes
No
80(7)
17(12)
1124
143